Introduction
The knee is the largest joint in the body and is critical for everyday functions like standing, walking and running. It is formed between three bones; the femur, tibia and patella, and is composed of two articulations; the tibiofemoral and patellofemoral joints. Keep reading to learn all about the anatomy of the knee, including its neovascular supply and lymphatic drainage. Pair this with our Knee Anatomy Revision Worksheets for the best revision experience.
Knee joint
The knee joint is a synovial joint that connects three bones; the femur, tibia and patella.
• The femur is the longest, heaviest and strongest bone in the human body
• The patella (kneecap) is the largest sesamoid bone in the human body
• The tibia is one of two bones that comprise the lower leg
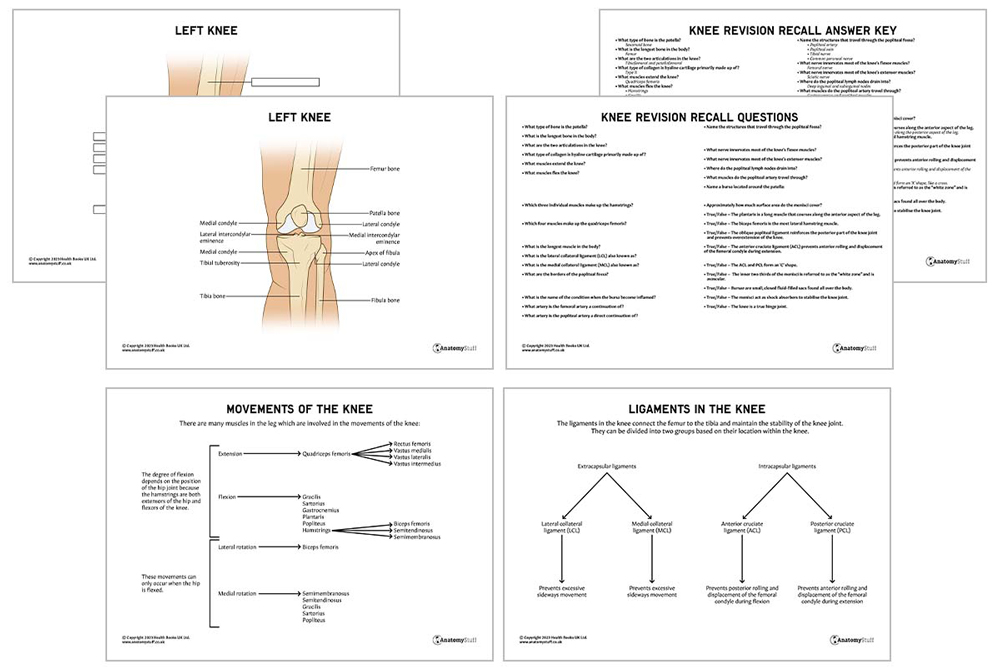
Two rounded joint surfaces are located at the lower end of the femur, the medial and lateral condyle, and they articulate smoothly with the tibia. The patella is located above these condyles and protects the anterior knee joint through its attachments to the quadriceps femoris tendon and patellar ligament. When the knee is bent or stretched, the patella slides along a groove in the femur.
A sesamoid bone is a bone embedded within a tendon or a muscle. They are found in the hand, knee, and foot.
Articulating Surfaces
An articulation is where two or more bones meet. Whilst most joints contain a single joint articulation, the knee consists of two: tibiofemoral (between the tibia and femur) and patellofemoral (between the femur and the patella). These surfaces are covered by a thick layer of hyaline cartilage which is primarily composed of type II collagen.
Collagens are the most abundant proteins in mammals.
Movements
The knee is a modified hinge joint, which permits flexion and extension. The degree of flexion depends on the position of the hip joint because the hamstrings are both extensors of the hip and flexors of the knee. For example, when the hip is flexed, the knee can flex up to 140°. However, when the hip is extended, the knee can only flex up to 120°.
The knee joint also has a rotational component which is why it is not a true hinge joint like the elbow. For example, when the hip is flexed, it can also facilitate lateral and medial rotation.
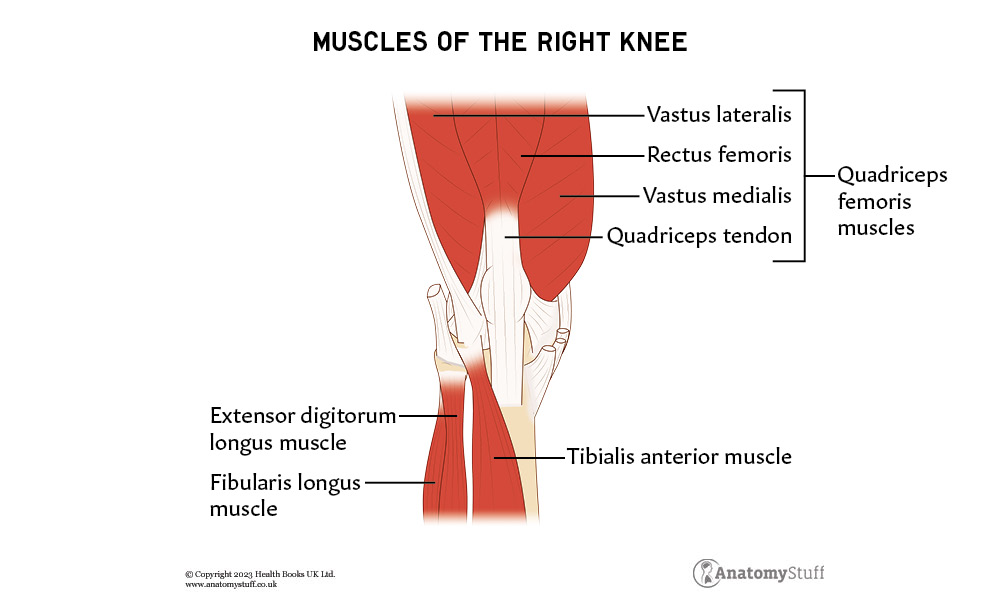
Muscles
There are many muscles in the leg which are involved in the movements of the knee:
| Movement | Muscle group |
| Extension | Quadriceps femoris – this is the strongest muscle in the human body and is located in the anterior compartment of the thigh. It consists of four individual muscles; three vastus muscles and the rectus femoris. They have different origins but conjoin to attach onto the patella as the quadriceps tendon.
|
| Flexion | Hamstrings – these are located in the posterior compartment of the thigh and consists of three individual muscles: the biceps femoris, semitendinosus and semimembranosus muscles.
Gracilis – a long, thin muscle located in the medial compartment of the thigh. Sartorius – the longest muscle in the body, spanning both the hip and the knee joints. Gastrocnemius – a large muscle located in the posterior compartment of the leg. Plantaris – a small muscle that courses along the posterior aspect of the leg. Popliteus – a small muscle that forms the floor of the popliteal fossa. |
| Lateral rotation | Biceps femoris – the most lateral hamstring muscle located in the posterior thigh. |
| Medial rotation | Semimembranosus – the most medial of the three hamstring muscles in the thigh.
Semitendinosus – a long superficial muscle in the back of the thigh. Gracilis Sartorius Popliteus |
Ligaments
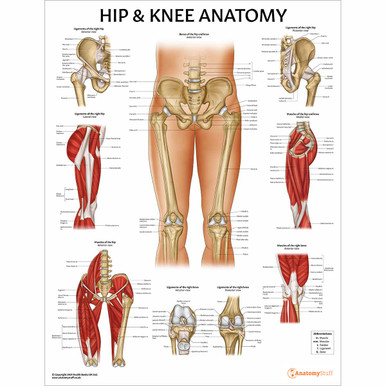
The ligaments in the knee connect the femur to the tibia and maintain the stability of the knee joint. They can be divided into two groups based on their location; extracapsular ligaments and intracapsular ligaments.
As the names suggest, the extracapsular ligaments can be found outside of the joint capsule and the intracapsular ligaments are located within the knee.
| Extracapsular ligaments | ||
| Ligament | Attachment sites | Function |
| Patellar ligament | A continuation of the quadriceps femoris tendon, which attaches onto the tibial tuberosity. | Stabilises the patella. |
| Lateral collateral ligament (LCL) | Lateral epicondyle of the femur and the head of the fibula. | Prevents excessive sideways movement. It is also known as the fibular collateral ligament. |
| Medial collateral ligament (MCL) | Medial epicondyle of the femur and the medial condyle of the tibia. | Prevents excessive sideways movement. It is also known as the tibial collateral ligament. |
| Oblique popliteal ligament | An extension of the semimembranosus tendon, which attaches on the lateral condyle of the femur. | Reinforces the posterior part of the knee joint and prevents overextension of the knee. |
| Arcuate popliteal ligament | Posterior aspect of the fibular head and the posterior side of the joint capsule of the knee. | Reinforces the posterolateral part of the knee joint and prevents overextension of the knee. |
| Intracapsular ligaments | ||
| Anterior cruciate ligament (ACL) | Lateral condyle of the femur and the intercondyloid eminence of the tibia. | Prevents posterior rolling and displacement of the femoral condyle during flexion. Also prevents hyperextension of the knee joint. |
| Posterior cruciate ligament (PCL) | Medial condyle of the femur and the posterior intercondylar area of the tibia. | Prevents anterior rolling and displacement of the femoral condyle during extension. Also prevents hyperflexion of the knee joint (opposite to ACL function). |
The collateral and cruciate ligaments are the four main stabilising ligaments of the knee. The ACL and PCL cross over each other and form an ‘X’ shape, like a cross. In Latin, ‘cruciate’ means cross.
Menisci
The medial and lateral menisci are two thick, C-shaped fibrocartilage structures. They are located between the articular surfaces of the tibia and femur, covering approximately 70% of its surface. They act as shock absorbers to stabilise the knee joint and distribute the weight of the body evenly.
The menisci are held in place by several ligaments, including the transverse ligament. The medial meniscus is attached at three points, compared to the lateral meniscus, which is only attached at two points. This means it does not move as freely as the lateral meniscus and, as a result, is torn more frequently.
The inner two-thirds of the menisci is called the “white zone” and is avascular. On the other hand, the outer third is known as the “red zone” and contains a rich blood supply via branches of the medial and lateral genicular arteries. This information is clinically significant, especially in the management of meniscal tears, which is a common injury.
Bursae
Bursae are small, closed, fluid-filled sacs found all over the body. They are most commonly found near the synovial membrane of the joints, and they act to reduce friction between adjacent moving structures. Bursae around the knee can be classified into two categories; those located around the patella and those found elsewhere.
Bursae around the patella:
• Prepatellar bursa
• Superficial and deep infrapatellar bursae
• Suprapatellar bursa
Bursae that are not anatomically close to the patella:
• Pes anserine bursa
• Iliotibial bursa
• Tibial and fibular collateral ligament bursae
• Gastrocnemius-semimembranosus bursa
When the bursa becomes inflamed, this is called bursitis. It is commonly due to trauma, infection or joint overuse.
![]()
Blood supply
The femoral and popliteal arteries supply the knee joint and its surrounding structures. The femoral artery begins just beyond the inguinal ligament and continues to the external iliac artery. It continues as the superficial femoral artery and gives off the deep femoral branch. The popliteal artery is a direct continuation of the superficial femoral artery.
The course of the popliteal artery:
- The popliteal artery continues the superficial femoral artery as it passes through the adductor magnus muscle’s adductor hiatus.
- It runs across and passes obliquely through the popliteal fossa, a diamond-shaped space posteriorly to the knee joint.
- It travels between the gastrocnemius and popliteal muscles of the posterior compartment of the leg.
- It bifurcates into the anterior and posterior tibial artery and the common trunk of the posterior tibial and peroneal arteries.
Geniculate arteries also branch off from multiple levels of the popliteal artery knee and contribute to collateral blood flow of the lower extremity:
• Superior lateral genicular artery
• Superior medial genicular artery
• Middle genicular artery
• Inferior lateral genicular artery
• Inferior medial genicular artery
The popliteal fossa has four major borders, which are formed from thigh and leg muscles located in the posterior compartment of the thigh:
• Superomedial border = semimembranosus and semitendinosus
• Superolateral border = biceps femoris
• Inferomedial border = medial head of gastrocnemius
• Inferolateral border = lateral head of gastrocnemius and plantaris
Several neurovascular structures enter and leave the leg through the popliteal fossa, including:
• Popliteal artery
• Popliteal vein
• Tibial nerve
• Common peroneal nerve
Innervation
The flexor muscles mainly receive innervation from branches of the femoral nerve, which is the largest branch of the lumbar plexus.
The extensor muscles receive innervation from the sciatic nerve, which arises from the sacral plexus.
Lymphatic drainage
The popliteal lymph nodes are found in the popliteal fossa. They drain most of the lymph from the knee and lower leg into the deep inguinal and subinguinal nodes.
Physiologic variants
Genu valgum, also known as ‘knocked knees’, is a lower leg deformity that exists when the knees turn inward. Genu varum, also known as ‘bowleg’, is when the legs curve outwards at the knees. These physiologic variants are considered to be a normal part of a child’s growth.
In conclusion, this comprehensive knee anatomy revision guide has taken you on a journey through the intricate and essential components of one of the body’s most complex joints. We’ve dissected the joint, ligaments, and muscles that make up the knee, and we’ve explored the functions and movement of the knee joint.

Related Products
View All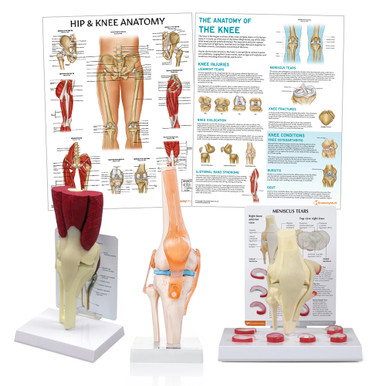

save
50%
AnatomyStuff
Knee Conditions Chart / Poster - Laminated
Now
£7.00
Inc VAT
Was
£14.00
Inc VAT