![]()
Introduction
The hip joint is the articulation between the acetabulum of the pelvis and the head of the femur. It is a ball and socket joint, providing a wide range of movement. It is also essential for weight-bearing and stability, facilitating important everyday tasks such as standing upright and rising from a chair. Keep reading to find out more about the anatomy of the hip joint, including its ligaments, neovascular supply and lymphatic drainage.
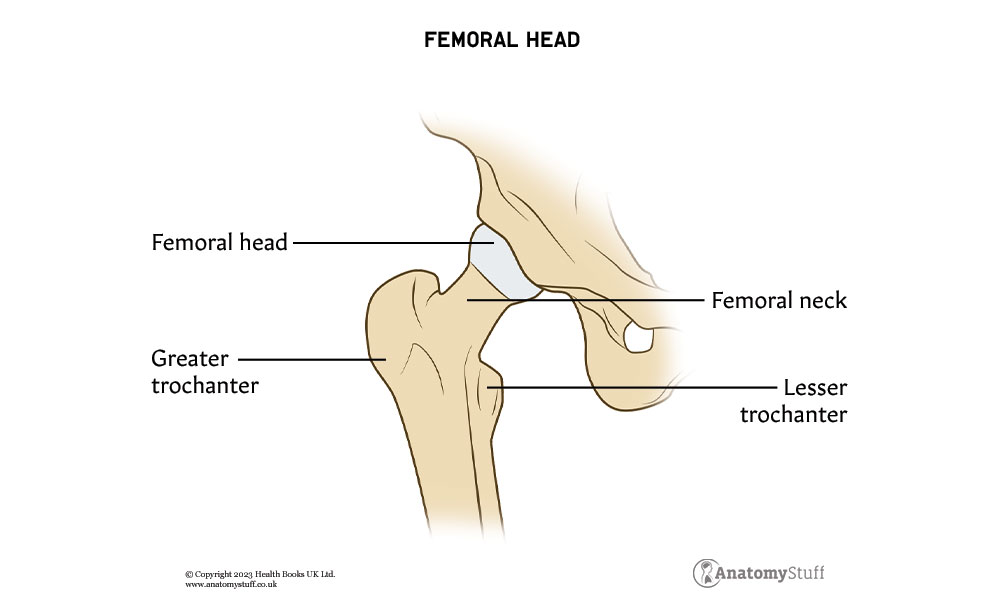
Head of femur
The femoral head is the highest part of the femur, and it articulates with the acetabulum of the pelvis. It is mostly spherical with a depression called the fovea capitis femoris in its centre. This is the site where the ligamentum teres attaches (discover more about the ligaments of the hip joint below). The femoral head is supported by the femoral neck, which contains 2 bony processes – the greater and lesser trochanters.
Acetabulum
The acetabulum is the ‘socket’ of the ‘ball and socket’ hip joint. It is a large, deep cavity formed by three pelvic bones, the ilium, ischium, and pubis. Approximately 40% of the femoral head is covered by the acetabulum at any one time.
Cartilage
Cartilage is a tough and fibrous tissue that acts as a shock absorber, enabling joints to move easily without friction. Part of the acetabulum, a ‘C’ shaped area called the lunate surface, is covered heavily by articular cartilage. This is the only part of the acetabulum in contact with the femoral head. The cartilage is found in layers approximately 2 – 4 mm thick and provides a smooth, lubricated surface.
The hip joint also contains a special type of cartilage called the labrum. This runs along the rim of the acetabulum, forming a tight and secure seal. It significantly increases the stability of the hip joint and reduces the chance of hip dislocation.
Interesting fact
In osteoarthritis, the articular cartilage is progressively broken down. Unfortunately, it has a limited capacity to repair itself, and this causes pain and mobility problems.
Bursae
The iliopsoas bursa is the largest in the body. In most adults, it is present bilaterally just below the iliopsoas muscle.
The trochanteric bursa is located on the lateral aspect of the hip. Due to its superficial position and proximity to large tendons, it can commonly become inflamed. When either the iliopsoas or trochanteric bursae become inflamed, this is called bursitis.
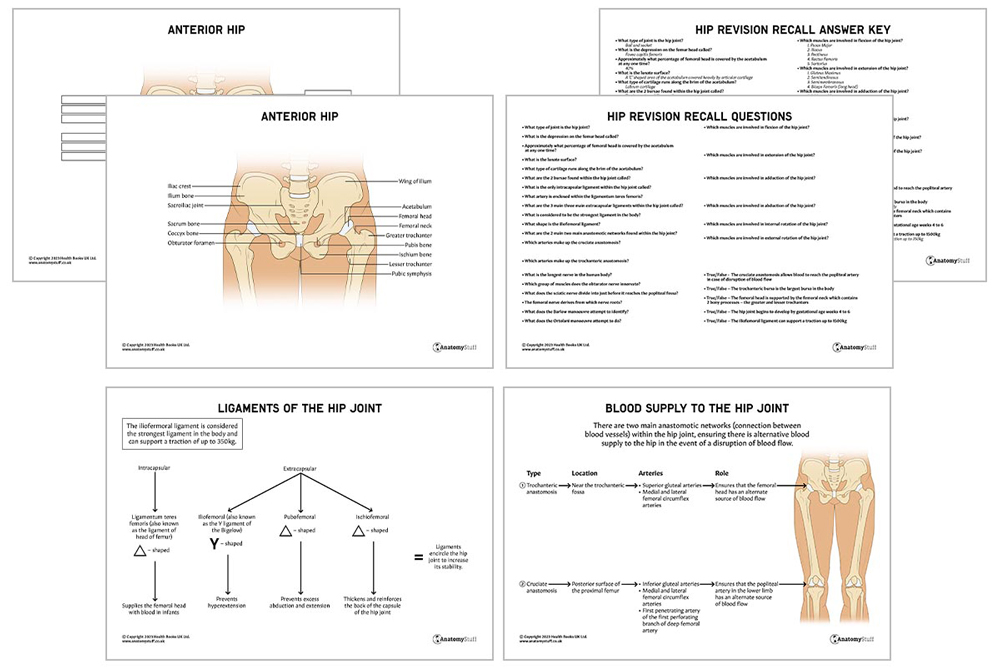
Ligaments
Ligaments (fibrous structures that connect bones to other bones) encircle the hip joint to increase its stability.
They can be divided into two groups – intracapsular and extracapsular.
Intracapsular:
The only intracapsular ligament within the hip joint is the ligament of the head of the femur, also known as ligamentum teres femoris. It connects the femoral head to the acetabulum and is thought to provide stability to the joint. The foveal artery (posterior branch of the obturator artery) is enclosed within this small ligament, supplying the femoral head with blood. This contribution is only significant in infants.
Extracapsular:
There are three main extracapsular ligaments which form a dense structure around the joint capsule.
|
Shape | Attachments | Function | |
| Iliofemoral (also known as the Y ligament of Bigelow) | Y-shaped | Anterior inferior iliac spine and the intertrochanteric crest of the femur | Prevents hyperextension
|
|
| Pubofemoral | Triangular | Superior pubic rami and the intertrochanteric line of the femur | Prevents excess abduction and extension | |
| Ischiofemoral | Triangular | Posterior surface of the acetabular rim and the anterior aspect of the femur | Thickens and reinforces the back of the capsule of the hip joint |
Interesting fact
The iliofemoral ligament is considered the strongest ligament in the body and can support traction up to 350kg.
![]()
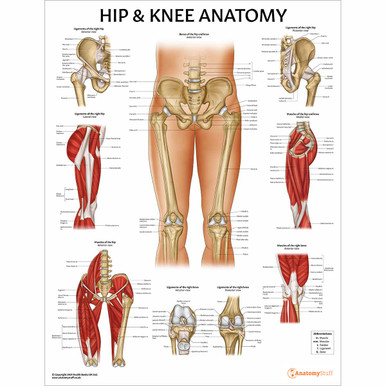
Muscles
Muscles of the hip joint can be categorised into different groups based on their function: flexion, extension, adduction, abduction, internal rotation and external rotation. Some muscles fall under several categories, such as the sartorius, the longest muscle in the human body, which runs down the length of the thigh.
| Flexion | Extension |
Adduction
|
Abduction
|
Internal Rotation
|
External Rotation
|
| Psoas Major
|
Gluteus Maximus
|
Adductor Magnus
|
Gluteus Medius
|
Tensor Fascia Latae
|
Gemellus Superior
|
| Iliacus
|
Semitendinosus
|
Adductor Longus
|
Tensor Fascia Latae
|
Gluteus Minimus
|
Gemellus Inferior
|
| Pectineus
|
Semimembranosus
|
Adductor Brevis
|
Sartorius | Obturator muscles | |
| Rectus Femoris
|
Biceps Femoris (long head)
|
Gracilis
|
Quadratus Femoris
|
||
| Sartorius | Pectineus
|
Gluteus maximus | |||
| Piriformis
|
|||||
| Sartorius |
Blood supply
The blood supply of the hip is relatively complex. The main arteries involved are:
• Obturator artery
• Medial and lateral femoral circumflex arteries
• Branches of the femoral artery
• Superior and inferior gluteal arteries.
Branches of these arteries form two main anastomotic networks, ensuring there is an alternative blood supply to the hip in the event of injury. This is extremely significant.
The first anastomotic network is called the cruciate anastomosis, which is located on the posterior surface of the proximal femur. It consists of the inferior gluteal arteries, the medial and lateral femoral circumflex arteries and the first penetrating artery of the first perforating branch of the deep femoral artery. This arterial network allows blood to reach the popliteal artery in the lower limb in case of disruption of blood flow between the external iliac and the femoral arteries.
The second major anastomosis is the trochanteric anastomosis which is located near the trochanteric fossa. It consists of the superior gluteal arteries and the medial and lateral femoral circumflex arteries. This anastomosis ensures that the femoral head has multiple alternate sources of blood flow if one or more arteries are injured or occluded.
Additionally, the blood supply to the hip varies with age. Between the ages of 0 to 4, the femoral head receives a significant blood supply from the medial and lateral femoral circumflex arteries and the ligament of the head of the femur, which carries the foveal artery (discussed above).
From the age of 4 onwards, the medial femoral circumflex artery provides the majority of the blood supply, and the contribution from the lateral femoral circumflex artery and the ligament of the head of the femur begins to decrease.
Damage to the medial circumflex femoral artery can result in avascular necrosis of the femoral head.
Nerve supply
The hip joint receives innervation from several different sources, including the sciatic, femoral and obturator nerves.
The sciatic nerve, derived from the lumbosacral plexus, is the longest nerve in the human body. It originates from nerve roots L4-S3, and it innervates a significant portion of the lower limb. Just before it reaches the popliteal fossa, it divides into the tibial nerve and the common peroneal nerve.
The femoral nerve is derived from nerve roots L2-L4. It is the largest branch of the lumbar plexus, and part of its role is to control the major hip flexor muscles.
The obturator nerve is derived from nerve roots L2-L4. It also arises from the lumbar plexus, and it provides innervation to all the hip adductors besides the hamstring part of the adductor magnus.
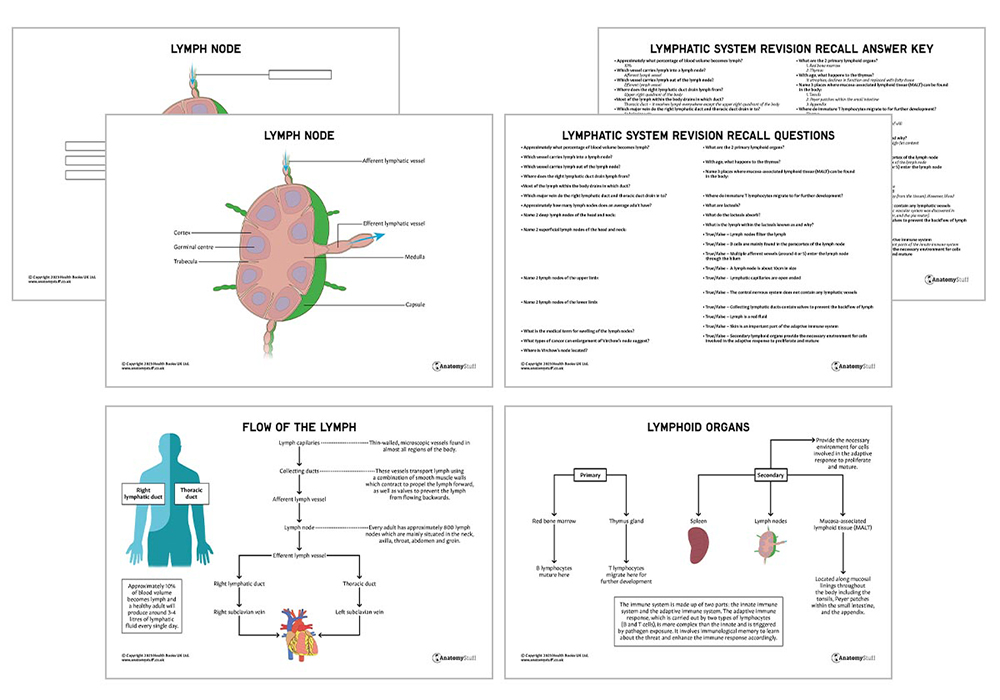
Lymphatic drainage
Lymphatic drainage from the anterior aspect of the hip joint drains to the deep inguinal nodes, which are found on the medial aspect of the femoral vein.
The medial and posterior aspects of the hip drain into the internal iliac nodes, which are located along the internal iliac arteries.
Check out our all-new Lymphatic System revision guide!
Embryology
The hip joint begins to develop by gestational age weeks 4 to 6. By week 7, a cleft develops between the precartilage cells. These are programmed to eventually form the femoral head and acetabulum. By 11 weeks of gestational age, the hip joint has mostly formed.
Interesting fact
Infants should have a full examination of the hip, including an assessment of hip joint instability. This is done by performing the Barlow and Ortolani tests (after 3 months of age, these become tests less sensitive). The Barlow manoeuvre involves identifying a dislocatable hip that can be pushed out of the socket with gentle posterior pressure. The Ortolani manoeuvre attempts to relocate a dislocated hip.

Related Products
View All


AnatomyStuff
Hip Anatomy Revision Worksheets (Interactive & Printable PDFs)
Now
£5.00
Inc VAT