Pressure Ulcer Care
Pressure ulcers (also called pressure sores, decubitus ulcers and bedsores) occur when the skin and underlying tissues become damaged from pressure, impairing blood supply.
They typically occur in people with reduced mobility and are subject to prolonged pressure or poor circulation, such as those confined to bed, immobile, elderly and people with diabetes and circulation problems.
Causes of Pressure Ulcers
Common causes include regular pressure on the site, shear, and friction. Patients sitting for most of the day, bedridden patients or those with reduced mobility and poor skin integrity are often at risk of developing pressure sores.
The following are warning indicators of bedsores or pressure ulcers:
• Colour of skin or texture changes
• Discharge of pus
• A part of the body that is colder or warmer to the touch than the rest of the body
• Tenderness to the touch.
Risk factors:
• Immobility: This might be caused by several factors, including chronic disease, spinal cord damage, etc.
• Impaired sensory perception: Sensory loss can be caused by spinal cord injuries, neurodegenerative disorders, peripheral vascular diseases, diabetes, and other disorders. It’s possible to ignore warning signs and the need to alter postures if the patient has lost their capacity to sense pain or discomfort.
• Dehydration: Dehydration diminishes the cushioning over bony points; those dehydrated are twice as prone to developing pressure ulcers.
• Incontinence
• Inadequate nourishment
• Obesity
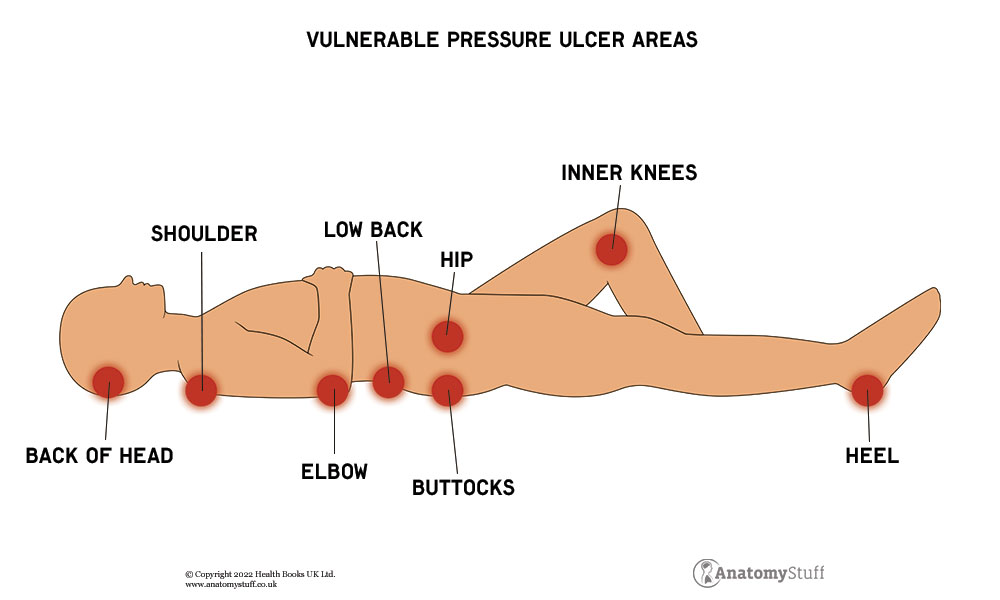
Vulnerable Pressure Ulcer Areas
Observing and monitoring the most likely sites of pressure sores is essential. Regular observation during repositioning and washing with the patient will alert you to early signs of pressure areas.
Areas of the body at risk are mainly over a bony prominence, such as the:
• Back of the head
• Ears
• Shoulder
• Elbow
• Low back
• Buttocks
• Hip
• Inner knees
• Heel
Free PDF Downloads
View All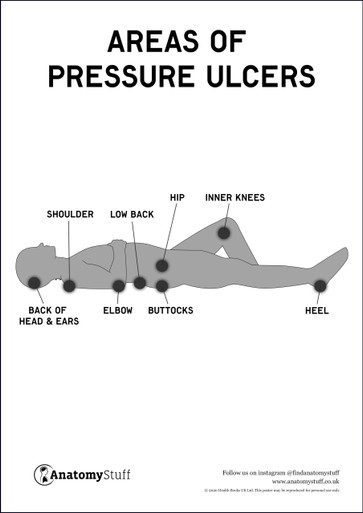
Assessment
To fully assess the patient, ensure they are informed and consent to a full assessment. The reason the assessment is so important is that when you look at the patient’s history, skin, pressure areas, and medications – (all of these can affect the development of an ulcer), it should give you a good indication as to whether or not they are likely to develop an ulcer – how much pressure their skin is under, and help you to put in place interventions early on Waterlow Pressure Sore Assessment Chart in order to prevent further damage to the skin.
For a full holistic assessment, include the following:
• Gain informed consent from the patient first
• Wash your hands
• Put sterile gloves on
• Explain the assessment to the patient
• Maintain the patient’s dignity and privacy
• Assess the patient holistically
• Assess using your clinical judgement and a validated scale such as Waterlow Score or the Norton risk-assessment scale, two well-recognised assessment tools.
• Assess for warning indicators of pressure ulcers such as the colour of skin or texture changes (red), warmer and tender to the touch.
Stages of a Pressure Ulcer
Pressure ulcers go through different stages; record and mark each stage appropriately according to your settings pressure area tool that is in place, e.g., Waterlow score etc.
Stage 1 The skin remains intact but is inflamed, red or purple and hot to the touch. Symptoms include a burning sensation, pain, and itchiness.
Stage 2 The skin is broken, presenting a shallow open ulcer. It may also present with painful blistering.
Stage 3 There is full-thickness tissue loss. The ulcer has a crater-like appearance and has extended to the subcutaneous fat layer. The wound may include undermining (erosion underneath the dermis layer). There is a high risk for infection.
Stage 4 Full-thickness tissue loss and the ulcer extend to the muscle, tendons or bone. There is often undermining and tunnelling of the skin. The risk for infection and sepsis is now significant.
Check out our Stages of Pressure Ulcers Chart to visually see stages 1-4.
Skin Inspection
Inspect the skin for temperature, colour, moisture, integrity, and turgor (elasticity). If there is an area of redness present, gently press down on it for 3 seconds, it should blanch, but the redness should return once you remove your finger. If the area remains white when you remove your finger, this indicates pressure damage in the underlying tissue. If left untreated, this can develop into a pressure ulcer.

Managing Pressure Ulcers
Pressure ulcers can be managed with pressure reduction, pain control, wound care and dressing, and infection prevention. Appropriate nutrition is also key in treating pressure ulcers.
Pressure reduction
Repositioning is the foremost step in addressing pressure ulcers. If you have a pressure ulcer, rotate, and alter positions often. Make sure to use mattresses composed of dynamic foam or those constructed of static foam, which aids in pressure relief. In addition, some mattresses contain a pump that keeps air flowing into the mattress steadily.
Pain killers and antibiotics
Non-Steroidal Anti-Inflammatory Drugs – NSAIDs are used to relieve pain during wound care and repositioning. Antibiotics may be required to prevent infection.
Wound Care and Dressing
When an ulcer is evident, record the anatomical position and measure the size of the wound, assess the wound’s dimensions, appearance, exudate and if any red sign of infection, odour, or pain is present.
Dress the wound per policy and the manufacturer’s directions for the dressing. Record (in the patient’s notes) the assessment and findings, measurements and date and initial the dressing.
If the skin isn’t damaged, wash it with a light clinical cleanser and allow it to dry. Wash the exposed wounds with water or a saline solution every time the bandage is replaced. A bandage speeds up the healing process and serves as an infection barrier.
Having dead or damaged tissue removed can aid in the healing of a sore.
If the pressure ulcer does not heal, surgery may be needed.
Prevention of Pressure Ulcers
You can try to prevent pressure ulcers by frequent repositioning to relieve skin pressure, a good skincare routine, healthy eating, proper hydration, avoiding smoking, and regular exercise.
You essentially want or relieve pressure/avoid consistent pressure, keep skin and body hydrated, avoid friction, moisture or shearing, and maintain good clinical observation for early indicators of ulcer development. You can help prevent pressure ulcers by ensuring the patient repositions regularly to relieve skin pressure. The use of pressure-relieving cushions, mattresses, chair pads and other supporting aids can help relieve pressure.
Repositioning advice:
At least once an hour, transfer the patient’s weight by repositioning them. Consider getting a wheelchair that is tailored to their needs and reduces pressure. Raise the bed to avoid shearing. If a significant bedsore does not heal, surgery may be required. One surgical restoration procedure is covering the wound and cushioning the damaged bone with a pad made of the patient’s muscle, skin, or other tissue.
Outlook
It’s advisable to take every precaution to avoid these pressure ulcers and to treat them as soon as they appear.